Neonatal hypoxia ischaemia (HI) is the third leading cause of neonatal death worldwide. Medical imaging plays an important role in its diagnosis and monitoring. We aim to analyze the clinical and ultrasound aspects of neonatal HI at the Ouahigouya Regional University Hospital (CHUR/OHG). This was an analytical cross-sectional study with retrospective data collection covering the period from 1 January 2017 to 30 April 2019. During the study period, neonatal HI for 20.12% of pediatric admissions, of which 33.7% underwent Transfontanellar ultrasound (7.31% of all ultrasounds). The sex ratio was 1.6. The majority (85.81%) of children were born at term. According to the Sarnat classification, mild distress predominated (66.89%), followed by moderate distress (27.03%) and severe distress (6.08%). Transfontanellar ultrasound was abnormal in 71 patients (47.97%). Typical brain lesions found were hemorrhage (27.70%), anoxic-ischaemic encephalopathy (18.24%), and periventricular leukomalacia (2.70%). The outcome was normal in 81.08% of patients, with a mortality rate of 6.08%. In view of the seriousness of neonatal brain damage, it is necessary to improve diagnostic methods (MRI) and treatment (hypothermia) to limit the sequelae.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Neonatal hypoxia ischaemia (HI), also known as perinatal asphyxia, is "fetal hypoxia with severe acidosis leading to poor cardiorespiratory adaptation at birth and, in the most serious cases, is accompanied by severe encephalopathy with multivisceral failure"
[1]
De Montgolfier I. Encéphalopathie hypoxo-ischémique du nouveau-né à terme Diagnostic, orientation et prise en charge. [Hypoxo-ischaemic encephalopathy of the new-born at term Diagnosis, referral and management]. Groupe Hospitalier Pitié Salpêtrière, Paris. JTA 2009. 13p.
[1]
. It is the third leading cause of neonatal mortality worldwide (23%), after low birth weight (30%) and neonatal infections (25%).
[2]
Kedy Koum D, Essomba N, Penda CI, Engome CB, Doumbe J, Mangamba LME, et al. Évolution des nouveau-nés à terme et près du terme hospitalisés pour asphyxie néonatale à l’Hôpital de district de Bonassama. [Outcome of term and near-term neonates hospitalised for neonatal asphyxia at Bonassama District Hospital]. Health Sci. Dis. 2018; 19 (2): 50-55.
. In developing countries, particularly in Africa, neonatal HI incidence is still high (42‰)
[3]
Ouédraogo/Yugbaré SO, Coulibaly G, Kouéta F, Yao S, Savadogo H, Dao L, et al. Profil à risque et pronostic néonatal de l’asphyxie périnatale en milieu hospitalier pédiatrique à Ouagadougou. [Risk profile and neonatal prognosis of perinatal asphyxia in paediatric hospitals in Ouagadougou]. J pédiatr puér. 2015; 28: 64-70.
due mostly to inadequate monitoring of pregnant women and inappropriate management of the mother and newborn in the delivery room
[4]
Okoko AR, Ekouya-Bowassa G, Moyen E, Togho-Abessou LC, Atanda HL, Moyen G. Asphyxie périnatale au centre hospitalier et universitaire de Brazzaville. [Perinatal asphyxia at university hospital of Brazzaville]. J pédiatr puér [En ligne]. 2016 Septembre [20/01/2020]; 6pages.
. In Burkina Faso, the hospital incidence of perinatal asphyxia was 19.8% based on data collected from 1 June to 30 November 2013 at the Charles de Gaulle Pediatric University Hospital Centre
[3]
Ouédraogo/Yugbaré SO, Coulibaly G, Kouéta F, Yao S, Savadogo H, Dao L, et al. Profil à risque et pronostic néonatal de l’asphyxie périnatale en milieu hospitalier pédiatrique à Ouagadougou. [Risk profile and neonatal prognosis of perinatal asphyxia in paediatric hospitals in Ouagadougou]. J pédiatr puér. 2015; 28: 64-70.
Medical imaging plays an important role in the diagnosis and monitoring of neonatal brain injury
[5]
Anthonioz C, Loisel D, Delorme B, Pasco-Papon A, Aube C, Caron C. Aspects IRM de l’encéphalopathie anoxo-ischémique du nouveau-né à terme et du prématuré. [MRI aspects of anoxic-ischemic encephalopathy of the term and premature newborn]. J Radiol. 2006; 87: 1651-70.
. Radiological exploration techniques for neonatal brain damage are almost exclusively transfontanellar ultrasound (TFUS) and magnetic resonance imaging (MRI). MRI is the reference method for detecting lesions encountered in hypoxic-ischaemic encephalopathy (HIE)
[5]
Anthonioz C, Loisel D, Delorme B, Pasco-Papon A, Aube C, Caron C. Aspects IRM de l’encéphalopathie anoxo-ischémique du nouveau-né à terme et du prématuré. [MRI aspects of anoxic-ischemic encephalopathy of the term and premature newborn]. J Radiol. 2006; 87: 1651-70.
. However, TFUS is the most widely available medical imaging modality in Africa and is becoming increasingly accessible, even in remote areas. TFUS thus constitutes the initial radiological assessment for cerebral exploration in newborns and plays a fundamental role in screening and monitoring various cerebral lesions
[6]
Berrada S, Maoulainine FMR, Abousaad A. L’apport de l’échographie transfontanellaire en néonatologie [thèse][The contribution of transfontanellar ultrasound in neonatology]. Médecine: Marrakech; 2012, 102p.
[7]
N’timon B, Gbande P, Dagbe M, Tchaou M, Amadou A, Sonhaye L, et al. Echographie pédiatrique en pratique hospitalière au Centre Hospitalier Universitaire (CHU) de Kara au Togo. [Paediatric ultrasound in hospital practice at the Centre Hospitalier Universitaire (CHU) de Kara in Togo]. Eur Sci J. 2018; 14(4): 443-53.
. To this end, we aimed to study the clinical aspects and contribution of this technique neonatal HI management at the Ouahigouya Regional University Hospital (CHUR-OHG).
2. Materials and Methods
The study was performed in the medical imaging and pediatric department of the CHUR-OHG.
This was an analytical cross-sectional study with retrospective data collection from 1er January 2017 to 30 April 2019.
All patients aged between 1 and 28 days, followed in the pediatric department of the CHUR-OHG during the study period with available clinical records and who had undergone an TFUS in the medical imaging department for neonatal HI were included.
Data were collected from ultrasound registers and patients' clinical records on a pre-established individual form. It included variables such as epidemiological data (age, sex, address), medical history (antenatal, perinatal, and postnatal), clinical data, TFUS indication, TFUS results, and other paraclinical data (hemogram results, erythrocyte sedimentation rate, C-reactive protein.
Data were analyzed using Epi info software. Chi-square and FISHER statistical tests were used to compare proportions at the 5% significance level.
Authorization from the Director General of the CHUR-OHG was obtained before the start of our study, and data were collected in such a way as to respect the anonymity of the patients.
3. Results
3.1. Epidemiological Data
During the 28-month study period, 534 newborns were admitted to the pediatric department for neonatal HI giving a rate of 20.12%. Of them, 61% were male giving a sex ratio of 1.6. Only 33.7% of 534 newborns with neonatal HI underwent TFUS. In the same period, 269 TFUS out of a total of 3649 ultrasound scans were performed in the CHUR-OHG medical imaging department, i.e. 7.37% of all ultrasound examinations. Neonatal HI was the indication of TFUS in 66.91% of cases.
The average age of newborns at admission to pediatric department was 2.5 days, with extremes of 1 and 18 days, and 7 days at TFUS realization with extremes of 1 and 28 days. The average time between admission to pediatrics and TFUS realization was 5 days.
3.2. Clinical Data
In relation to antenatal history, the number of antenatal consultations (ANCs) varied between 0 to 6, and 89.19% of mothers had attended more than 3 ANCs. Newborns from pregnancies that had undergone at least 4 ANC accounted for 57.43%. The mean term of pregnancy was 37 weeks of amenorrhoea (WA)), with extremes of 25 WA and 44 WA. and 10.14% were multiple. In terms of perinatal history, 89.86% of pregnancies were singleton and 17.57% of delivery were by cesarean. The mean birth weight was 2905 grams, with extremes of 1200 grams and 4800 grams. The APGAR score was below 7 in 75.68% of newborns at 1 minute and 54.05% at 5minutes. In this study, 65.54% of newborns received resuscitation at birth, with an average resuscitation time of 9 minutes and extremes of 3 and 36 minutes. The nature of the amniotic fluid was specified in 84.46% of patients, with a predominance of meconium (37.6%).
The reasons of hospitalization were dominated by respiratory distress (50%) followed by reflex abnormalities (26%). According to the Sarnat classification, grade I was predominant (66.89%) in our patients, followed by grade II (27.03%) and grade III (6.08%).
3.3. Ultrasound Data
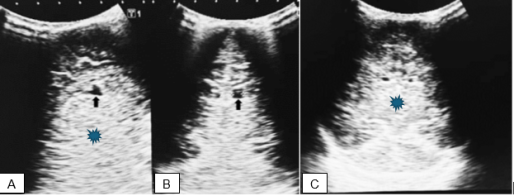
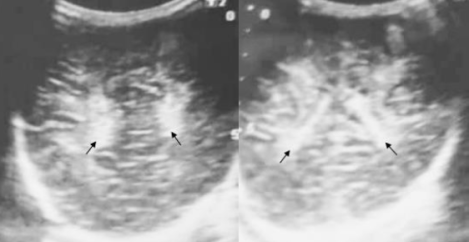
The TFUS result was pathological in 47.97% of cases. There were 27.7% of hemorrhages, 18.24% of hypoxo-ischaemic encephalopathy, and 2.7% of periventricular leukomalacia (Figures 1-3). Cerebral hemorrhage was found mostly in term newborns (27.7% / 21.62%) as well as for hypoxo-ischaemic encephalopathy (18.24% / 15.53%). However, periventricular leukomalacia seemed to be more common in premature babies (2,03% / 2.70%).
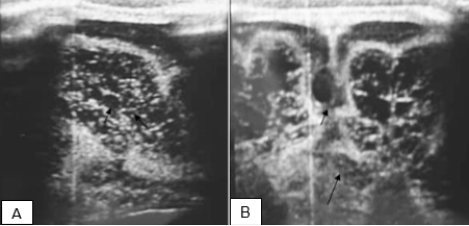
Figure 3. Sagittal (A) and coronal (B) ultrasound sections in a 7-day-old full-term boy, showing hypoxo-ischemic encephalopathy with multicystic encephaloma made up of numerous wallless anechoic images with tendency to confluence, disseminated in the cerebral parenchyma (arrows).
The presence of global abnormalities at TFUS was significantly associated with the Sarnat stage with p value = 0.02 (table 1), and more specifically the presence of hypoxo-ischaemic encephalopathy with p value = 0.0008 (table 2).
Table 1. TFUS abnormality according to Sarnat stage.
Parameters
number of people
Abnormal ETF
P-value
odds ratio
Confidence Interval
Sarnat
0,02
0,46
[0,23-0,92]
2-3
49
30 (61,22%)
1
99
42 (42,42%)
Table 2. Sarnat stage according to hypoxo-ischaemic encephalopathy.
Parameters
number of people
Sarnat stade 2-stade 3
P-value
odds ratio
Confidence Interval
Hypoxic-ischaemic encephalopathy
0,0008
0,23
[0,09-0,55]
Oui
28
17 (60,71%)
Non
120
32 (26,67%)
3.4. Evolution
The average length of hospitalization was 10 days, with extremes of 1 and 34 days.
Discharge from hospital was normal in 81.08% newborns and 6.08% of deaths were recorded.
Mortality was significantly associated with the Sarnat stage with p value = 0.0006 (table 3).
Table 3. Mortality prognosis according to Sarnat stage.
Parameters
Lethality
number of people
P-value
odds ratio
Confidence Interval
Sarnat
0,0006
0,05
[0,006-0,04]
Stade 2-stade 3
8 (16,33%)
49
Stade 1
1 (1,01%)
99
4. Discussion
4.1. Epidemiological Data
In our study, perinatal asphyxia accounted for 20.12% of neonatal admissions to CHUR-OHG. Our results are similar to those reported by Ouédraogo/Yugbaré SO
[3]
Ouédraogo/Yugbaré SO, Coulibaly G, Kouéta F, Yao S, Savadogo H, Dao L, et al. Profil à risque et pronostic néonatal de l’asphyxie périnatale en milieu hospitalier pédiatrique à Ouagadougou. [Risk profile and neonatal prognosis of perinatal asphyxia in paediatric hospitals in Ouagadougou]. J pédiatr puér. 2015; 28: 64-70.
Thiam L, Dramé A, Coly IZ, Diouf FN, Sylla A, Ndiaye O. Asphyxie périnatale au service de néonatologie de l’hôpital de la Paix De Ziguinchor (Sénégal). [Perinatal asphyxia in the neonatology department of the Hôpital de la Paix in Ziguinchor (Senegal)]. European Sci J. 2017; 13(21): 217-26.
(20,6%). TFUS accounted for 7.31% of all medical imaging scans. This rate is higher than that of N'timon B
[7]
N’timon B, Gbande P, Dagbe M, Tchaou M, Amadou A, Sonhaye L, et al. Echographie pédiatrique en pratique hospitalière au Centre Hospitalier Universitaire (CHU) de Kara au Togo. [Paediatric ultrasound in hospital practice at the Centre Hospitalier Universitaire (CHU) de Kara in Togo]. Eur Sci J. 2018; 14(4): 443-53.
which was 1.6%. The policy of free care for newborns and pregnant women would explain this relatively high TFUS realization in our context.
The average age of newborns at admission was 2.5 days. This result was close to that of Okoko AR
[4]
Okoko AR, Ekouya-Bowassa G, Moyen E, Togho-Abessou LC, Atanda HL, Moyen G. Asphyxie périnatale au centre hospitalier et universitaire de Brazzaville. [Perinatal asphyxia at university hospital of Brazzaville]. J pédiatr puér [En ligne]. 2016 Septembre [20/01/2020]; 6pages.
i.e. 2.7 days. Other African authors such as Fiangoa F
[9]
Fiangoa F, Raveloharimino H, Andriatahiana T, Soukkainatte S, Rabesandratana HN. Profil épidémio-clinique et pronostic à court terme de l’asphyxie périnatale vue au CHU Mahajanga. [Epidemiological and clinical profile and short-term prognosis of perinatal asphyxia at the Mahajanga University Hospital]. Rev Malg Pédiatr. 2018; 1(1): 88-96.
[9]
and Ouédraogo/Yugbaré SO
[3]
Ouédraogo/Yugbaré SO, Coulibaly G, Kouéta F, Yao S, Savadogo H, Dao L, et al. Profil à risque et pronostic néonatal de l’asphyxie périnatale en milieu hospitalier pédiatrique à Ouagadougou. [Risk profile and neonatal prognosis of perinatal asphyxia in paediatric hospitals in Ouagadougou]. J pédiatr puér. 2015; 28: 64-70.
reported a lower average ages with 1.2 days and 1.7 days respectively. The fact that some newborns often pass through several health centers before reaching the CHUR-OHG, the referral hospital for the northern region of Burkina Faso, would justify the high mean age at admission in pediatric department.
Men predominated (61%). Fiangoa F
[9]
Fiangoa F, Raveloharimino H, Andriatahiana T, Soukkainatte S, Rabesandratana HN. Profil épidémio-clinique et pronostic à court terme de l’asphyxie périnatale vue au CHU Mahajanga. [Epidemiological and clinical profile and short-term prognosis of perinatal asphyxia at the Mahajanga University Hospital]. Rev Malg Pédiatr. 2018; 1(1): 88-96.
[9]
(57.42%) and Ouédraogo /Yugbaré SO
[3]
Ouédraogo/Yugbaré SO, Coulibaly G, Kouéta F, Yao S, Savadogo H, Dao L, et al. Profil à risque et pronostic néonatal de l’asphyxie périnatale en milieu hospitalier pédiatrique à Ouagadougou. [Risk profile and neonatal prognosis of perinatal asphyxia in paediatric hospitals in Ouagadougou]. J pédiatr puér. 2015; 28: 64-70.
(62.4%) also reported male dominance. According to Badawi N
[10]
Badawi N, Kurinczuk JJ, Keogh JM, Alessandri LM, O’Sullivan F, Burton PR et al. Antepartum risk factors for moderate to severe neonatal hypoxic ischemic encephalopathy: a swedish national cohort study. AOGS. 2018; 97: 615-23.
reported that sex hormones, in particular estrogens, protect against anoxic-ischaemic lesions.
4.2. Clinical Data
Newborns from pregnancies that received at least 4 ANC accounted for 57.43%. Fiangoa F
[9]
Fiangoa F, Raveloharimino H, Andriatahiana T, Soukkainatte S, Rabesandratana HN. Profil épidémio-clinique et pronostic à court terme de l’asphyxie périnatale vue au CHU Mahajanga. [Epidemiological and clinical profile and short-term prognosis of perinatal asphyxia at the Mahajanga University Hospital]. Rev Malg Pédiatr. 2018; 1(1): 88-96.
[9]
and Okoko AR
[4]
Okoko AR, Ekouya-Bowassa G, Moyen E, Togho-Abessou LC, Atanda HL, Moyen G. Asphyxie périnatale au centre hospitalier et universitaire de Brazzaville. [Perinatal asphyxia at university hospital of Brazzaville]. J pédiatr puér [En ligne]. 2016 Septembre [20/01/2020]; 6pages.
recorded rates was higher than our results with respectively 74% and 80.8%. The WHO recommends monitoring pregnancies with at least 4 ANC. The late consultation at the first ANC would explain this difference and urges us to raise mothers' awareness of ANC, which remains ineffective. Most of our newborns (77.70%), like those of Siva Saranappa SB
[12]
Siva Saranappa S B, Chaithanya C Nair, Madhu G N, Srinivasa S, Manjunath MN. Clinical profile and outcome of perinatal asphyxia in a tertiary care centre. Curr Pediatr Res. 2015; 19(1 & 2): 9-12.
[12]
i.e. 80.34% and Lebbardi O
[13]
Lebbardi O, Aboussad A. La souffrance néonatale. Expérience du service de Néonatologie CHU Mohammed VI, Marrakech [Neonatal suffering. Experience of the Neonatology Department, Mohammed VI University Hospital, Marrakech] [Thèse]. Médecine: Marrakech; 2010, 3p.
[13]
i.e. 81.4%, were born at term. In our series, the majority of patients (82.43%) were born vaginally, as in the study by Ouédraogo/Yugbaré SO
[3]
Ouédraogo/Yugbaré SO, Coulibaly G, Kouéta F, Yao S, Savadogo H, Dao L, et al. Profil à risque et pronostic néonatal de l’asphyxie périnatale en milieu hospitalier pédiatrique à Ouagadougou. [Risk profile and neonatal prognosis of perinatal asphyxia in paediatric hospitals in Ouagadougou]. J pédiatr puér. 2015; 28: 64-70.
also in Burkina Faso. Elsewhere in Africa and the world, Nihal AK
[14]
Nihal AK, Barkat A. L’asphyxie périnatale au centre de médecine et de réanimation néonatales- FMP Rabat. [Perinatal asphyxia at the neonatal medicine and resuscitation centre - FMP RABAT]. Int J Med Health Sci. 2018; 4: 31-41.
Siva Saranappa S B, Chaithanya C Nair, Madhu G N, Srinivasa S, Manjunath MN. Clinical profile and outcome of perinatal asphyxia in a tertiary care centre. Curr Pediatr Res. 2015; 19(1 & 2): 9-12.
[12]
, and Sidibé LN
[15]
Sidibé LN, Diall H, Konaté D, Coulibaly O, Diakité FL, Sacko K, et al. Epidemio-Clinical Characteristics of Perinatal Anoxia and Immediate Outcome of Patients at Hospital Teaching Gabriel Touré of Bamako. Open Journal of Pediatrics. 2019, 9: 326-336.
reported respectively 74.8%, 75%, and 76% of vaginal deliveries. Most of the patients (78.38%) had a normal birth weight with an average of 2905 g. This average weight is close to that of Sidibé LN
[15]
Sidibé LN, Diall H, Konaté D, Coulibaly O, Diakité FL, Sacko K, et al. Epidemio-Clinical Characteristics of Perinatal Anoxia and Immediate Outcome of Patients at Hospital Teaching Gabriel Touré of Bamako. Open Journal of Pediatrics. 2019, 9: 326-336.
Lebbardi O, Aboussad A. La souffrance néonatale. Expérience du service de Néonatologie CHU Mohammed VI, Marrakech [Neonatal suffering. Experience of the Neonatology Department, Mohammed VI University Hospital, Marrakech] [Thèse]. Médecine: Marrakech; 2010, 3p.
[13]
which are 2876 g and 2900 g respectively. Pregnancy follow-up, with more than half of the women having undergone at least 4 ANC, could explain the high rate of newborns with normal weights. Most patients (70.4%) had an abnormal amniotic fluid at birth. Fiangoa F
[9]
Fiangoa F, Raveloharimino H, Andriatahiana T, Soukkainatte S, Rabesandratana HN. Profil épidémio-clinique et pronostic à court terme de l’asphyxie périnatale vue au CHU Mahajanga. [Epidemiological and clinical profile and short-term prognosis of perinatal asphyxia at the Mahajanga University Hospital]. Rev Malg Pédiatr. 2018; 1(1): 88-96.
[9]
, Thiam L
[8]
Thiam L, Dramé A, Coly IZ, Diouf FN, Sylla A, Ndiaye O. Asphyxie périnatale au service de néonatologie de l’hôpital de la Paix De Ziguinchor (Sénégal). [Perinatal asphyxia in the neonatology department of the Hôpital de la Paix in Ziguinchor (Senegal)]. European Sci J. 2017; 13(21): 217-26.
Ouédraogo/Yugbaré SO, Coulibaly G, Kouéta F, Yao S, Savadogo H, Dao L, et al. Profil à risque et pronostic néonatal de l’asphyxie périnatale en milieu hospitalier pédiatrique à Ouagadougou. [Risk profile and neonatal prognosis of perinatal asphyxia in paediatric hospitals in Ouagadougou]. J pédiatr puér. 2015; 28: 64-70.
also reported a predominance of the abnormal nature of amniotic fluid with respectively 74.1%, 77.22%, and 78%. For Diarra KL
[16]
Diarra KL. La souffrance foetale aiguë dans le service de gynéco obstétrique du CHU Gabriel-Touré. [Acute foetal distress in the obstetrics and gynaecology department of the CHU Gabriel-Touré] [Thèse]. Médecine. Bamako. 2008, 108p.
[16]
, there is a significant link between stained or meconium amniotic fluid and perinatal asphyxia. According to Bordarier C
[17]
Bordarier C. Souffrance cérébrale asphyxique du nouveau-né à terme. [Cerebral asphyxia in term newborns]. Encycl Méd-Chir. (Elsevier Masson, Paris), pédiatrie-Maladie infectieuse, 4002-S-60, 2002, 36p.
[17]
, hypoxia is responsible for an increased intestinal peristalsis and relaxation of the anal sphincter by sympathetic stimulation, resulting in meconium emission.
4.3. Ultrasound Data
In our series, TFUS results were predominantly normal (52.03%). Likewise, Ouédraogo/Yugbaré SO
[3]
Ouédraogo/Yugbaré SO, Coulibaly G, Kouéta F, Yao S, Savadogo H, Dao L, et al. Profil à risque et pronostic néonatal de l’asphyxie périnatale en milieu hospitalier pédiatrique à Ouagadougou. [Risk profile and neonatal prognosis of perinatal asphyxia in paediatric hospitals in Ouagadougou]. J pédiatr puér. 2015; 28: 64-70.
Lebbardi O, Aboussad A. La souffrance néonatale. Expérience du service de Néonatologie CHU Mohammed VI, Marrakech [Neonatal suffering. Experience of the Neonatology Department, Mohammed VI University Hospital, Marrakech] [Thèse]. Médecine: Marrakech; 2010, 3p.
[13]
(80%), and Okoko AR
[4]
Okoko AR, Ekouya-Bowassa G, Moyen E, Togho-Abessou LC, Atanda HL, Moyen G. Asphyxie périnatale au centre hospitalier et universitaire de Brazzaville. [Perinatal asphyxia at university hospital of Brazzaville]. J pédiatr puér [En ligne]. 2016 Septembre [20/01/2020]; 6pages.
(91%) reported mostly normal results. This could be explained by the fact that clinical distress is not always reflected by ultrasound lesions. In addition, TFUS is not always sensitive, especially when lesions are minor and/or symmetrical and requiring MRI realization. TFUS revealed cerebral hemorrhages with 27.70%. This was also the most frequent lesion (32%) observed by Berrada S
[6]
Berrada S, Maoulainine FMR, Abousaad A. L’apport de l’échographie transfontanellaire en néonatologie [thèse][The contribution of transfontanellar ultrasound in neonatology]. Médecine: Marrakech; 2012, 102p.
[6]
. Hypoxo-ischaemic encephalopathy accounted for 18.24% of lesions. Berrada S
[6]
Berrada S, Maoulainine FMR, Abousaad A. L’apport de l’échographie transfontanellaire en néonatologie [thèse][The contribution of transfontanellar ultrasound in neonatology]. Médecine: Marrakech; 2012, 102p.
[6]
and Ouédraogo/Yugbaré SO
[3]
Ouédraogo/Yugbaré SO, Coulibaly G, Kouéta F, Yao S, Savadogo H, Dao L, et al. Profil à risque et pronostic néonatal de l’asphyxie périnatale en milieu hospitalier pédiatrique à Ouagadougou. [Risk profile and neonatal prognosis of perinatal asphyxia in paediatric hospitals in Ouagadougou]. J pédiatr puér. 2015; 28: 64-70.
had much lower rates, 2.3% and 3.5% respectively. Periventricular leukomalacia was present in 2.70% of newborns. This frequency is lower than that of Berrada S
[6]
Berrada S, Maoulainine FMR, Abousaad A. L’apport de l’échographie transfontanellaire en néonatologie [thèse][The contribution of transfontanellar ultrasound in neonatology]. Médecine: Marrakech; 2012, 102p.
[6]
(3.9%) and Ouédraogo/Yugbaré SO
[3]
Ouédraogo/Yugbaré SO, Coulibaly G, Kouéta F, Yao S, Savadogo H, Dao L, et al. Profil à risque et pronostic néonatal de l’asphyxie périnatale en milieu hospitalier pédiatrique à Ouagadougou. [Risk profile and neonatal prognosis of perinatal asphyxia in paediatric hospitals in Ouagadougou]. J pédiatr puér. 2015; 28: 64-70.
(5,9%). These differences in results are related to the variability of neonatal hypoxia ischaemia lesions.
4.4. Evolution
The average hospital stay was 10 days. This average is identical to that of Thiam L
[8]
Thiam L, Dramé A, Coly IZ, Diouf FN, Sylla A, Ndiaye O. Asphyxie périnatale au service de néonatologie de l’hôpital de la Paix De Ziguinchor (Sénégal). [Perinatal asphyxia in the neonatology department of the Hôpital de la Paix in Ziguinchor (Senegal)]. European Sci J. 2017; 13(21): 217-26.
and close to those of Ouédraogo/Yugbaré SO (11.7 days)
[3]
Ouédraogo/Yugbaré SO, Coulibaly G, Kouéta F, Yao S, Savadogo H, Dao L, et al. Profil à risque et pronostic néonatal de l’asphyxie périnatale en milieu hospitalier pédiatrique à Ouagadougou. [Risk profile and neonatal prognosis of perinatal asphyxia in paediatric hospitals in Ouagadougou]. J pédiatr puér. 2015; 28: 64-70.
Somé MJM, Tankoano AI, Ouedraogo PA, Ackra YE, Jacquemin C, Suzanne A, Tayeb M, Egreteau L, Lougue CL. Apport de l’imagerie par résonance magnétique dans la prise en charge de la souffrance cérébrale néonatale. [The contribution of magnetic resonance imaging in the management of neonatal cerebral distress]. Health Sci. Dis: 2021; 22(1): 57-61.
(13.5 days). There were 10.81% of discharges against medical advice. Fiangoa F
[9]
Fiangoa F, Raveloharimino H, Andriatahiana T, Soukkainatte S, Rabesandratana HN. Profil épidémio-clinique et pronostic à court terme de l’asphyxie périnatale vue au CHU Mahajanga. [Epidemiological and clinical profile and short-term prognosis of perinatal asphyxia at the Mahajanga University Hospital]. Rev Malg Pédiatr. 2018; 1(1): 88-96.
[9]
reported 7.92%. This could be due to the poverty of the population. We recorded a relatively high mortality rate (6.08%) as for Ouédraogo/Yugbaré SO
[3]
Ouédraogo/Yugbaré SO, Coulibaly G, Kouéta F, Yao S, Savadogo H, Dao L, et al. Profil à risque et pronostic néonatal de l’asphyxie périnatale en milieu hospitalier pédiatrique à Ouagadougou. [Risk profile and neonatal prognosis of perinatal asphyxia in paediatric hospitals in Ouagadougou]. J pédiatr puér. 2015; 28: 64-70.
Siva Saranappa S B, Chaithanya C Nair, Madhu G N, Srinivasa S, Manjunath MN. Clinical profile and outcome of perinatal asphyxia in a tertiary care centre. Curr Pediatr Res. 2015; 19(1 & 2): 9-12.
[12]
(8%) and Thiam L
[8]
Thiam L, Dramé A, Coly IZ, Diouf FN, Sylla A, Ndiaye O. Asphyxie périnatale au service de néonatologie de l’hôpital de la Paix De Ziguinchor (Sénégal). [Perinatal asphyxia in the neonatology department of the Hôpital de la Paix in Ziguinchor (Senegal)]. European Sci J. 2017; 13(21): 217-26.
Neonatal hypoxia ischaemia is a worrying pathology, and its frequency remains high at the CHUR-OHG. The FTUS, which is of great help in diagnosing and monitoring this condition, is normal in most cases in our study. The lesions found were, in order of frequency, hemorrhage, hypoxo-ischaemic encephalopathy, and periventricular leukomalacia. To improve the prognosis of this condition, regular monitoring of pregnancies and labor delivery under better conditions, availability of high-performance imaging equipment (FTUS, MRI) and appropriate neonatal management using hypothermia are essential.
Abbreviations
ANC: Antenatal consultation
CHUR/OHG: Ouahigouya Regional University Hospital
CRP: C-reactive protein
ESR: Erythrocyte sedimentation rate
HI: Hypoxia ischaemia
HIE: Hypoxic-ischaemic encephalopathy
MRI: Magnetic resonance imaging
TFUS: Transfontanellar ultrasound
WA: Weeks of amenorrhoea
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
De Montgolfier I. Encéphalopathie hypoxo-ischémique du nouveau-né à terme Diagnostic, orientation et prise en charge. [Hypoxo-ischaemic encephalopathy of the new-born at term Diagnosis, referral and management]. Groupe Hospitalier Pitié Salpêtrière, Paris. JTA 2009. 13p.
[2]
Kedy Koum D, Essomba N, Penda CI, Engome CB, Doumbe J, Mangamba LME, et al. Évolution des nouveau-nés à terme et près du terme hospitalisés pour asphyxie néonatale à l’Hôpital de district de Bonassama. [Outcome of term and near-term neonates hospitalised for neonatal asphyxia at Bonassama District Hospital]. Health Sci. Dis. 2018; 19 (2): 50-55.
Ouédraogo/Yugbaré SO, Coulibaly G, Kouéta F, Yao S, Savadogo H, Dao L, et al. Profil à risque et pronostic néonatal de l’asphyxie périnatale en milieu hospitalier pédiatrique à Ouagadougou. [Risk profile and neonatal prognosis of perinatal asphyxia in paediatric hospitals in Ouagadougou]. J pédiatr puér. 2015; 28: 64-70.
Okoko AR, Ekouya-Bowassa G, Moyen E, Togho-Abessou LC, Atanda HL, Moyen G. Asphyxie périnatale au centre hospitalier et universitaire de Brazzaville. [Perinatal asphyxia at university hospital of Brazzaville]. J pédiatr puér [En ligne]. 2016 Septembre [20/01/2020]; 6pages.
Anthonioz C, Loisel D, Delorme B, Pasco-Papon A, Aube C, Caron C. Aspects IRM de l’encéphalopathie anoxo-ischémique du nouveau-né à terme et du prématuré. [MRI aspects of anoxic-ischemic encephalopathy of the term and premature newborn]. J Radiol. 2006; 87: 1651-70.
Berrada S, Maoulainine FMR, Abousaad A. L’apport de l’échographie transfontanellaire en néonatologie [thèse][The contribution of transfontanellar ultrasound in neonatology]. Médecine: Marrakech; 2012, 102p.
[7]
N’timon B, Gbande P, Dagbe M, Tchaou M, Amadou A, Sonhaye L, et al. Echographie pédiatrique en pratique hospitalière au Centre Hospitalier Universitaire (CHU) de Kara au Togo. [Paediatric ultrasound in hospital practice at the Centre Hospitalier Universitaire (CHU) de Kara in Togo]. Eur Sci J. 2018; 14(4): 443-53.
Thiam L, Dramé A, Coly IZ, Diouf FN, Sylla A, Ndiaye O. Asphyxie périnatale au service de néonatologie de l’hôpital de la Paix De Ziguinchor (Sénégal). [Perinatal asphyxia in the neonatology department of the Hôpital de la Paix in Ziguinchor (Senegal)]. European Sci J. 2017; 13(21): 217-26.
Fiangoa F, Raveloharimino H, Andriatahiana T, Soukkainatte S, Rabesandratana HN. Profil épidémio-clinique et pronostic à court terme de l’asphyxie périnatale vue au CHU Mahajanga. [Epidemiological and clinical profile and short-term prognosis of perinatal asphyxia at the Mahajanga University Hospital]. Rev Malg Pédiatr. 2018; 1(1): 88-96.
[10]
Badawi N, Kurinczuk JJ, Keogh JM, Alessandri LM, O’Sullivan F, Burton PR et al. Antepartum risk factors for moderate to severe neonatal hypoxic ischemic encephalopathy: a swedish national cohort study. AOGS. 2018; 97: 615-23.
Siva Saranappa S B, Chaithanya C Nair, Madhu G N, Srinivasa S, Manjunath MN. Clinical profile and outcome of perinatal asphyxia in a tertiary care centre. Curr Pediatr Res. 2015; 19(1 & 2): 9-12.
[13]
Lebbardi O, Aboussad A. La souffrance néonatale. Expérience du service de Néonatologie CHU Mohammed VI, Marrakech [Neonatal suffering. Experience of the Neonatology Department, Mohammed VI University Hospital, Marrakech] [Thèse]. Médecine: Marrakech; 2010, 3p.
[14]
Nihal AK, Barkat A. L’asphyxie périnatale au centre de médecine et de réanimation néonatales- FMP Rabat. [Perinatal asphyxia at the neonatal medicine and resuscitation centre - FMP RABAT]. Int J Med Health Sci. 2018; 4: 31-41.
Sidibé LN, Diall H, Konaté D, Coulibaly O, Diakité FL, Sacko K, et al. Epidemio-Clinical Characteristics of Perinatal Anoxia and Immediate Outcome of Patients at Hospital Teaching Gabriel Touré of Bamako. Open Journal of Pediatrics. 2019, 9: 326-336.
Diarra KL. La souffrance foetale aiguë dans le service de gynéco obstétrique du CHU Gabriel-Touré. [Acute foetal distress in the obstetrics and gynaecology department of the CHU Gabriel-Touré] [Thèse]. Médecine. Bamako. 2008, 108p.
[17]
Bordarier C. Souffrance cérébrale asphyxique du nouveau-né à terme. [Cerebral asphyxia in term newborns]. Encycl Méd-Chir. (Elsevier Masson, Paris), pédiatrie-Maladie infectieuse, 4002-S-60, 2002, 36p.
[18]
Somé MJM, Tankoano AI, Ouedraogo PA, Ackra YE, Jacquemin C, Suzanne A, Tayeb M, Egreteau L, Lougue CL. Apport de l’imagerie par résonance magnétique dans la prise en charge de la souffrance cérébrale néonatale. [The contribution of magnetic resonance imaging in the management of neonatal cerebral distress]. Health Sci. Dis: 2021; 22(1): 57-61.
Marouruana, S. M. J., Ali, O. P., Ida, T. A., Adama, S., Bassirou, K., et al. (2024). Clinical and Ultrasound Aspects of Neonatal Hypoxia Ischaemia at the Regional University Hospital of Ouahigouya. International Journal of Medical Imaging, 12(1), 16-21. https://doi.org/10.11648/j.ijmi.20241201.14
Marouruana, S. M. J.; Ali, O. P.; Ida, T. A.; Adama, S.; Bassirou, K., et al. Clinical and Ultrasound Aspects of Neonatal Hypoxia Ischaemia at the Regional University Hospital of Ouahigouya. Int. J. Med. Imaging2024, 12(1), 16-21. doi: 10.11648/j.ijmi.20241201.14
Marouruana SMJ, Ali OP, Ida TA, Adama S, Bassirou K, et al. Clinical and Ultrasound Aspects of Neonatal Hypoxia Ischaemia at the Regional University Hospital of Ouahigouya. Int J Med Imaging. 2024;12(1):16-21. doi: 10.11648/j.ijmi.20241201.14
@article{10.11648/j.ijmi.20241201.14,
author = {Some Milckisédek Judicaël Marouruana and Ouedraogo Pakisba Ali and Tankoano Aïda Ida and Savadogo Adama and Kindo Bassirou and Ouermi Alain Saga and Ouedraogo Nina-Astrid and Bamouni Yomboé Abel and Diallo Ousseini},
title = {Clinical and Ultrasound Aspects of Neonatal Hypoxia Ischaemia at the Regional University Hospital of Ouahigouya
},
journal = {International Journal of Medical Imaging},
volume = {12},
number = {1},
pages = {16-21},
doi = {10.11648/j.ijmi.20241201.14},
url = {https://doi.org/10.11648/j.ijmi.20241201.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmi.20241201.14},
abstract = {Neonatal hypoxia ischaemia (HI) is the third leading cause of neonatal death worldwide. Medical imaging plays an important role in its diagnosis and monitoring. We aim to analyze the clinical and ultrasound aspects of neonatal HI at the Ouahigouya Regional University Hospital (CHUR/OHG). This was an analytical cross-sectional study with retrospective data collection covering the period from 1 January 2017 to 30 April 2019. During the study period, neonatal HI for 20.12% of pediatric admissions, of which 33.7% underwent Transfontanellar ultrasound (7.31% of all ultrasounds). The sex ratio was 1.6. The majority (85.81%) of children were born at term. According to the Sarnat classification, mild distress predominated (66.89%), followed by moderate distress (27.03%) and severe distress (6.08%). Transfontanellar ultrasound was abnormal in 71 patients (47.97%). Typical brain lesions found were hemorrhage (27.70%), anoxic-ischaemic encephalopathy (18.24%), and periventricular leukomalacia (2.70%). The outcome was normal in 81.08% of patients, with a mortality rate of 6.08%. In view of the seriousness of neonatal brain damage, it is necessary to improve diagnostic methods (MRI) and treatment (hypothermia) to limit the sequelae.
},
year = {2024}
}
TY - JOUR
T1 - Clinical and Ultrasound Aspects of Neonatal Hypoxia Ischaemia at the Regional University Hospital of Ouahigouya
AU - Some Milckisédek Judicaël Marouruana
AU - Ouedraogo Pakisba Ali
AU - Tankoano Aïda Ida
AU - Savadogo Adama
AU - Kindo Bassirou
AU - Ouermi Alain Saga
AU - Ouedraogo Nina-Astrid
AU - Bamouni Yomboé Abel
AU - Diallo Ousseini
Y1 - 2024/04/02
PY - 2024
N1 - https://doi.org/10.11648/j.ijmi.20241201.14
DO - 10.11648/j.ijmi.20241201.14
T2 - International Journal of Medical Imaging
JF - International Journal of Medical Imaging
JO - International Journal of Medical Imaging
SP - 16
EP - 21
PB - Science Publishing Group
SN - 2330-832X
UR - https://doi.org/10.11648/j.ijmi.20241201.14
AB - Neonatal hypoxia ischaemia (HI) is the third leading cause of neonatal death worldwide. Medical imaging plays an important role in its diagnosis and monitoring. We aim to analyze the clinical and ultrasound aspects of neonatal HI at the Ouahigouya Regional University Hospital (CHUR/OHG). This was an analytical cross-sectional study with retrospective data collection covering the period from 1 January 2017 to 30 April 2019. During the study period, neonatal HI for 20.12% of pediatric admissions, of which 33.7% underwent Transfontanellar ultrasound (7.31% of all ultrasounds). The sex ratio was 1.6. The majority (85.81%) of children were born at term. According to the Sarnat classification, mild distress predominated (66.89%), followed by moderate distress (27.03%) and severe distress (6.08%). Transfontanellar ultrasound was abnormal in 71 patients (47.97%). Typical brain lesions found were hemorrhage (27.70%), anoxic-ischaemic encephalopathy (18.24%), and periventricular leukomalacia (2.70%). The outcome was normal in 81.08% of patients, with a mortality rate of 6.08%. In view of the seriousness of neonatal brain damage, it is necessary to improve diagnostic methods (MRI) and treatment (hypothermia) to limit the sequelae.
VL - 12
IS - 1
ER -
Marouruana, S. M. J., Ali, O. P., Ida, T. A., Adama, S., Bassirou, K., et al. (2024). Clinical and Ultrasound Aspects of Neonatal Hypoxia Ischaemia at the Regional University Hospital of Ouahigouya. International Journal of Medical Imaging, 12(1), 16-21. https://doi.org/10.11648/j.ijmi.20241201.14
Marouruana, S. M. J.; Ali, O. P.; Ida, T. A.; Adama, S.; Bassirou, K., et al. Clinical and Ultrasound Aspects of Neonatal Hypoxia Ischaemia at the Regional University Hospital of Ouahigouya. Int. J. Med. Imaging2024, 12(1), 16-21. doi: 10.11648/j.ijmi.20241201.14
Marouruana SMJ, Ali OP, Ida TA, Adama S, Bassirou K, et al. Clinical and Ultrasound Aspects of Neonatal Hypoxia Ischaemia at the Regional University Hospital of Ouahigouya. Int J Med Imaging. 2024;12(1):16-21. doi: 10.11648/j.ijmi.20241201.14
@article{10.11648/j.ijmi.20241201.14,
author = {Some Milckisédek Judicaël Marouruana and Ouedraogo Pakisba Ali and Tankoano Aïda Ida and Savadogo Adama and Kindo Bassirou and Ouermi Alain Saga and Ouedraogo Nina-Astrid and Bamouni Yomboé Abel and Diallo Ousseini},
title = {Clinical and Ultrasound Aspects of Neonatal Hypoxia Ischaemia at the Regional University Hospital of Ouahigouya
},
journal = {International Journal of Medical Imaging},
volume = {12},
number = {1},
pages = {16-21},
doi = {10.11648/j.ijmi.20241201.14},
url = {https://doi.org/10.11648/j.ijmi.20241201.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmi.20241201.14},
abstract = {Neonatal hypoxia ischaemia (HI) is the third leading cause of neonatal death worldwide. Medical imaging plays an important role in its diagnosis and monitoring. We aim to analyze the clinical and ultrasound aspects of neonatal HI at the Ouahigouya Regional University Hospital (CHUR/OHG). This was an analytical cross-sectional study with retrospective data collection covering the period from 1 January 2017 to 30 April 2019. During the study period, neonatal HI for 20.12% of pediatric admissions, of which 33.7% underwent Transfontanellar ultrasound (7.31% of all ultrasounds). The sex ratio was 1.6. The majority (85.81%) of children were born at term. According to the Sarnat classification, mild distress predominated (66.89%), followed by moderate distress (27.03%) and severe distress (6.08%). Transfontanellar ultrasound was abnormal in 71 patients (47.97%). Typical brain lesions found were hemorrhage (27.70%), anoxic-ischaemic encephalopathy (18.24%), and periventricular leukomalacia (2.70%). The outcome was normal in 81.08% of patients, with a mortality rate of 6.08%. In view of the seriousness of neonatal brain damage, it is necessary to improve diagnostic methods (MRI) and treatment (hypothermia) to limit the sequelae.
},
year = {2024}
}
TY - JOUR
T1 - Clinical and Ultrasound Aspects of Neonatal Hypoxia Ischaemia at the Regional University Hospital of Ouahigouya
AU - Some Milckisédek Judicaël Marouruana
AU - Ouedraogo Pakisba Ali
AU - Tankoano Aïda Ida
AU - Savadogo Adama
AU - Kindo Bassirou
AU - Ouermi Alain Saga
AU - Ouedraogo Nina-Astrid
AU - Bamouni Yomboé Abel
AU - Diallo Ousseini
Y1 - 2024/04/02
PY - 2024
N1 - https://doi.org/10.11648/j.ijmi.20241201.14
DO - 10.11648/j.ijmi.20241201.14
T2 - International Journal of Medical Imaging
JF - International Journal of Medical Imaging
JO - International Journal of Medical Imaging
SP - 16
EP - 21
PB - Science Publishing Group
SN - 2330-832X
UR - https://doi.org/10.11648/j.ijmi.20241201.14
AB - Neonatal hypoxia ischaemia (HI) is the third leading cause of neonatal death worldwide. Medical imaging plays an important role in its diagnosis and monitoring. We aim to analyze the clinical and ultrasound aspects of neonatal HI at the Ouahigouya Regional University Hospital (CHUR/OHG). This was an analytical cross-sectional study with retrospective data collection covering the period from 1 January 2017 to 30 April 2019. During the study period, neonatal HI for 20.12% of pediatric admissions, of which 33.7% underwent Transfontanellar ultrasound (7.31% of all ultrasounds). The sex ratio was 1.6. The majority (85.81%) of children were born at term. According to the Sarnat classification, mild distress predominated (66.89%), followed by moderate distress (27.03%) and severe distress (6.08%). Transfontanellar ultrasound was abnormal in 71 patients (47.97%). Typical brain lesions found were hemorrhage (27.70%), anoxic-ischaemic encephalopathy (18.24%), and periventricular leukomalacia (2.70%). The outcome was normal in 81.08% of patients, with a mortality rate of 6.08%. In view of the seriousness of neonatal brain damage, it is necessary to improve diagnostic methods (MRI) and treatment (hypothermia) to limit the sequelae.
VL - 12
IS - 1
ER -